It was the perfect storm: a complicated pregnancy, a high intervention labor, and then, on top of it all, she was having trouble breastfeeding. This already exhausted mother was at her wit's end, but I knew how committed she was to making it work.
I weighed her baby and examined her breasts. Baby's weight down. Very sleepy. Mom's breasts displaying the classic symptoms: wide spaced, tubular, no report of changes during pregnancy. I calmly told her I think she has insufficient glandular tissue (IGT), and she almost immediately burst into tears.
She could barely get her words out, but after a moment I realized she was crying not because of the diagnosis, but because of the validation. Someone somewhere, on a message board or what have you, had told her IGT isn't a real thing, that it's an excuse for women who don't want to put the work into breastfeeding. I shook my head and reaffirmed my previous statement: "Insufficient glandular tissue is very real." "Thank you," she said, and asked what to do about it.
What It Is
Insufficient glandular tissue, or hypoplasia, is one of the leading causes of primary lactation failure (failure to produce enough milk even though the baby's latch and suck are normal). While severity of IGT varies from person to person, an estimated
1 in 1000 mothers have IGT severe enough to preclude a full milk supply despite "doing everything right."
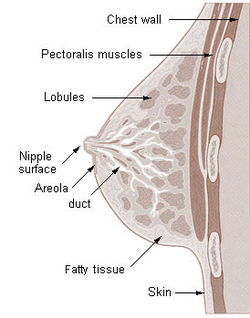 |
Image sourced at
http://en.wikipedia.org/wiki/Mammary_gland |
Everyone develops the basis for functional breast tissue (milk sacks, ducts, etc) during the embryonic stage regardless of sex. During puberty, increased levels of estrogen cue the creation of extra fat, connective tissue, and some functional tissue. Pregnancy hormones ignite the proliferation of functional tissue: ducts, milk sacks, etc; by about the 16th week of pregnancy, the breast is a functioning gland.
Those with IGT, however, have experienced an interruption in this process. While the exact cause is unknown, it is believed that this interruption takes place during puberty, whereby the body fails to develop the basis for glandular tissue. Without this basis, the breasts cannot adequately create and release milk.
This is not to say they will not produce
some milk. Many mothers with IGT have the ability to produce breastmilk, just in insufficient quantities to sustain their babies. Again, severity varies from person to person, and treatment plans will vary based on severity as well as infant patterns.
What It Looks Like
The "typical" hypoplastic breasts will be tubular instead of rounded. They may be widely spaced, one
may be larger than the other. Some display a marked swelling in the areola. This image shows varying breast shapes; note varying markers of hypoplasia in types 2-4:
 |
| Image sourced at http://www.sallychapman.net/2013/05/hypoplasia.html |
Many young women note during their teenage years that their breasts don't "hang" the way they should. While this is not a definitive symptom of IGT, it is a good idea to discuss concerns with a lactation consultant during pregnancy, especially if you have experienced little or no breast changes during pregnancy.
Why It Happens
It's not clear what, exactly, causes insufficient glandular tissue, but there are theories. Some experts believe genetic components may be at play. IGT expert Diana Cassar-Uhl suggests
luteal phase defects may be a common cause: inadequate progesterone certainly could preclude the development of functional breast tissue.
Others believe PCOS, obesity, a history of disordered eating, and other factors that alter hormone levels may prohibit sufficient development of glandular tissue.
What It Isn't
IGT is a lot of things. A few things it is not:
- The same thing as having small breasts. Contrary to popular belief, small breasts do not, in fact, make breastfeeding more difficult. While women with smaller breasts have less storage capacity (and therefore may feed their babies more often), small breasts alone do not preclude the ability to make enough milk. While IGT mamas often have smaller breasts, hypoplasia is found across the spectrum of breast sizes.
- A cop out/all in your head. I think I've put this myth to rest by now, yes? It's real, folks.
- The end of your breastfeeding relationship. This is the biggest concern for IGT mothers, and while results vary, there are many things you can do to get the most milk for your baby. Many supplement their babies while breastfeeding, often all at once at the breast with a supplementer. And formula is not your only option: many families are able to access informally donated breastmilk in their communities to help sustain their little ones.
Treatment and Support
Since no two mothers are alike, the care plans for IGT vary from person to person. Seeing a lactation consultant during pregnancy (yes, before baby is even born!) will help you understand whether or not your breasts appear hypoplastic and give you a plan of action for when the baby comes. Then the best idea is to monitor signs of adequate intake and commence treatment for IGT as soon as you notice a problem. This may include herbs, prescription drugs, supplementation, frequent weight checks, etc.
After receiving clinical care from a lactation consultant, the most important thing is to surround yourself with support! There are countless mothers out there with IGT; finding a community with shared experiences is key to staying positive and feeling good about yourself and your infant feeding decisions.
noteveryonecanbreastfeed.com has an amazing
resource list, and I definitely recommend checking out the
IGT and Low Milk Supply Support group on Facebook.
Lauren Guy
CD(DONA), IBCLC







